
Page 9 - GUIAS ESC ESH 2018
P. 9
ESC/ESH Guidelines 9
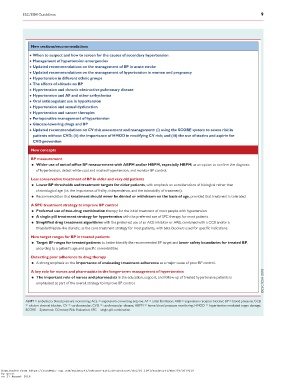
New sections/recommendations
When to suspect and how to screen for the causes of secondary hypertension
Management of hypertension emergencies
Updated recommendations on the management of BP in acute stroke
Updated recommendations on the management of hypertension in women and pregnancy
Hypertension in different ethnic groups
The effects of altitude on BP
Hypertension and chronic obstructive pulmonary disease
Hypertension and AF and other arrhythmias
Oral anticoagulant use in hypertension
Hypertension and sexual dysfunction
Hypertension and cancer therapies
Perioperative management of hypertension
Glucose-lowering drugs and BP
Updated recommendations on CV risk assessment and management: (i) using the SCORE system to assess risk in
patients without CVD; (ii) the importance of HMOD in modifying CV risk; and (iii) the use of statins and aspirin for
CVD prevention
New concepts
BP measurement
• Wider use of out-of-office BP measurement with ABPM and/or HBPM, especially HBPM, as an option to confirm the diagnosis
of hypertension, detect white-coat and masked hypertension, and monitor BP control.
Less conservative treatment of BP in older and very old patients
• Lower BP thresholds and treatment targets for older patients, with emphasis on considerations of biological rather than
chronological age (i.e. the importance of frailty, independence, and the tolerability of treatment).
• Recommendation that treatment should never be denied or withdrawn on the basis of age, provided that treatment is tolerated.
A SPC treatment strategy to improve BP control
• Preferred use of two-drug combination therapy for the initial treatment of most people with hypertension.
• A single-pill treatment strategy for hypertension with the preferred use of SPC therapy for most patients.
• Simplified drug treatment algorithms with the preferred use of an ACE inhibitor or ARB, combined with a CCB and/or a
thiazide/thiazide-like diuretic, as the core treatment strategy for most patients, with beta-blockers used for specific indications.
New target ranges for BP in treated patients
• Target BP ranges for treated patients to better identify the recommended BP target and lower safety boundaries for treated BP,
according to a patient’s age and specific comorbidities.
Detecting poor adherence to drug therapy
• A strong emphasis on the importance of evaluating treatment adherence as a major cause of poor BP control.
A key role for nurses and pharmacists in the longer-term management of hypertension
• The important role of nurses and pharmacists in the education, support, and follow-up of treated hypertensive patients is
emphasized as part of the overall strategy to improve BP control.
ABPM = ambulatory blood pressure monitoring; ACE = angiotensin-converting enzyme; AF = atrial fibrillation; ARB = angiotensin receptor blocker; BP = blood pressure; CCB
= calcium channel blocker; CV = cardiovascular; CVD = cardiovascular disease; HBPM = home blood pressure monitoring; HMOD = hypertension-mediated organ damage;
SCORE = Systematic COronary Risk Evaluation; SPC = single-pill combination.
Downloaded from https://academic.oup.com/eurheartj/advance-article-abstract/doi/10.1093/eurheartj/ehy339/5079119
by guest
on 27 August 2018